






Shafeeque Ahmed1*, Shama2, Gani MA3, Najam Sultana4, Khamrunissa Shaikh5
1Department of Saidla–wo- Murakbath, Tipu Sultan Unani Medical College & Hosptal, Gulbaga, Karnataka, India.
2Government AYUSH Hospital, Manvi, Dist Raichur, India.
3Department of Ilmul Amraz, Tipu Sultan Unani Medical College & Hosptal, Gulbaga, Karnataka, India.
4Department of Moalijat, Tipu Sultan Unani Medical College & Hosptal, Gulbaga, Karnataka, India.
5Ibn Sina National College for Medical Studies, Jeddah, KSA.
ORIGINAL RESEARCH ARTICLE
Volume 3, Issue 2, Page 80-83, May-August 2015.
Article history
Received: 10 July 2015
Revised: 3 August 2015
Accepted: 5 August 2015
Early view: 11 August 2015
*Author for correspondence
E-mail: [email protected]
Background: Hyperlipidemia is a major health problem in today’s era. In Unani System of medicine many drugs are available both single as well as compound formulations. Sharbat–e-Qalbi, a compound formulation, is a reliable Unani medicine by legendary Unani physician Hkm. Mohammed Adam Ali Khardi in Gulbarga District (for more than 40 years). According to him, this medicine is very beneficial for Amraz-e-Qalb (Heart diseases), Ziqutud dum Qawi (Hypertension), Saman-e-Mufrat (Obesity) etc.
Material and methods: It is a clinical study on Azdiyad-e-Shahmiya (Hyperlipidemia), a single blind study on 30 patients. The main objective was to evaluate and observe the effect of Shar-bat-e-Qalbi in the management of Azdiyad-e-Shahmiya (Hyperlipidemia).
Results: This medicine was found to be highly significant in lowering the level of cholesterol, triglycerides, low density lipoproteins and in increasing the level of high density lipoproteins in cases of primary hyperlipidemia.
Conclusion: This compound formulation is very useful in maintaining lipid profile in optimum range.
Keywords: Unani Medicine, Azdiyad-e-Shahmiya (Hyperlipidemia), Sharbat-e-Qalbi.
INTRODUCTION
Hyperlipidemia is an important risk factor for coronary artery disease. Therefore lowering increased cholesterol is crucial for primary and secondary prevention. Nutritive management and drug treatment is frequently needed to lower the cholesterol in the serum (Schaefer, 2003).
Hyperlipidemia is a major metabolic disorder vastly seen in this era of modernization and fast life, living through stressful life and fast foods having high calories and also has every comfort of living and physical inactivity. A group of supplementary metabolic risk is-sues are often found in association with this Hyperlipidemia together with obesity, Glucose intolerance, hypertension & insulin resistance (Rihana & Shagufta 2009). The concept of hyerlipidemia is based on the biochemical variations in blood i.e. altered lipid metabolism cause increased level of lipids in the blood (Boyer Rodney 2002).
Unani physicians have reported that the presence in blood from Dosoomat of blood or from the oily substance of blood reaches the different body organs; it starts to accumulate as fat (Shaham) (Abdul Nasir et al., 2013). As there is lack of knowledge in biochemical test, Unani physicians at that time were unable to explain it.
In this scientific era, hyperlipidemia and obesity are considered as two miscellaneous disorders, but they are connected with each other. The hyperlipidemia shows higher levels of lipids in blood (Rihana & Aleem 2009; Cristie & Rone, 2003).
Indians as a race are highly prone to premature atherosclerosis and coronary heart dis-ease. Likely that dyslipidemia might be one of the major contributors of this epidemic of Coronary Artery Disease and associated metabolic disorders.
Hyperlipidemia is usually due to the deranged digestion and metabolism. An accurate reference of hyperlipidemia is unavailable in Unani literature, but it can be known in terms of Dosoomat. Unani system of medicine strongly assumes that one of the major factors causes of every disease is diet of a person (Nafees, 1954).
This is happening mainly due to improper digestion of food by the effect of heavy diet. Hence the usage of drugs having the properties likes munafis-e-balgum, jaali, etc. (Hakim Kabiruddin, 2000; Hkm Kabeeruddin, 1935; Allama Hakim, 2011). There is an indigenous compound like safoof, sharbat, jawarish, majoon, habb etc. are having these properties (Hkm Kabeeruddin 1935, Ziur-Rehman 1991). The aim and objective of present study is to effectively manage the cases of hyperlipidemia with total herbal medicine, cost effective, easily available and with no unwanted effects i.e., Sharbat-e-Qalbi.
This Sharbat-e-Qalbi is a compound formulation of 5 unani medicines i.e., Zanjabil (Zingiber officinale), Laisan (Allium sativum), Limbu (Citrus aurantrifolia), Seeb ka Sirka (Malus syivestris) and Shahed (Apis Mellifera) in the dosage of 5ml twice before meals (Al-lama Hakim 2011, Hakim Kabiruddin 2000).
Ancient physicians were well aware of presence of lipids in the name of dasoomat which is present in blood. Increased blood lipid level had a injurious effect, as described in the background of obesity (Saman-e-Mufrat). This dasoomat is applied for the lipids of plas-ma (Cholestrol and triglycerides) and increased levels of which leads to hyperlipdiemia.
In the light of Unani literature, many of Unani Physicians and researchers have briefly described the condition of obesity under the name of ‘Saman-e-Mufrat’ which is almost similar to hyperlipidemia in all aspect as in etiology, clinical features, complications and management (Ibn Sina 2010).
Ali Ibn-e-Abbas Majoosi (930 AD) in his book ‘Kamil-e-sana’ told that “hararat-e-ghareezi” of such persons is less and blood vessels of his body are narrow & compressed. According to him life span of such persons is less because of their low “hararat-e-ghareezi” and narrow blood vessels the concentration of Rooh (Oxygen) in their blood is not sufficient, and also there is excess amount of vicious matter present in their bodies.
Abu Sahel Maseehi (970-1010 AD), describes Fat are of two types (Hakeem Mo-hammed Bin Zakariya Razi, 1999).
1. Sameen: it is soft, semisolid and has less property to solidify.
2. Shaham: It is hard and is found in the body adherent to kidneys.
Sameen and Shaham are formed in blood which has the property of dasoomat (oily sub-stance). According to Unani Literature the causes and complications are Khilqi saman-e-mufrat, Martoob-e-aghazia, farhat, rahat, sarwat, kasrat-e-ghiza, lack of riyazat, naram libaz, Murat-tab-e-roghaniyat, tukhama, kasrat-e-sharab noshi (Hakeem Mohammed Bin Zakariya Razi 1999, Nafees 1906).
The ancient Unani literature, there are description of many drugs both single and compound formulations used for the purpose of reducing body weight and treating obesity. Zanjabil (Zingiber officinale rose), Laisan (Allium sativum Linn), Limbu (Citrus aurantrifolia), Seeb ka Sirka (Malus syivestris mill) & Shahed (Apis mellifera) are among these drugs. As these medications are advantageous in obesity, also that can be proved beneficial in treatment of hyperlipidemia (Hakim Mohammed Abdul Hakim 2002, Allama Hakim 2011, Hakim Kabiruddin 2000).
MATERIALS AND METHODS
To evaluate and observe the effect of Sharbat-e-Qalbi in the management of primary hyperlipidemia, a study was design as a single blind clinical study on 30 cases between the age groups 30-60 years of either sex were selected from Tipu Sultan Unani Medical College and Teaching Hospital, Gulbarga, India. Patients were selected incidentally based on pathological evaluation are included in the study. Patients less than 30 & more than 60 years, or having Zanthoma, Xanthelesma, premature arcus, corne, symptoms of Ischemic Heart Disease (IHD), Patients with complex obesity, Patients with obligating history of Ischemic Heart Disease or Pregnant woman or taking any medicine which increase the level of lipids such as oral contraceptives pills (OCP), β- blockers and thiazinde diuretic etc were excluded. Patients were carefully selected for lipid profile was asked to attend department of Ilmul Amraz in a 12-14 hours fasting state (water permitted). Sharbat-e-Qalbi was prepared in the Department of Sadla-wa-Murakabat with standardized procedures. After that the medication is supplied to the department of Moalijat. Shabart-e-Qalbi is given in dose of 5ml twice in a day with hot water before meals. Patients were informed about the duration of the study and extra criteria. Study was carried out about 90 days.
The data were collected and tabulated. The collected data was statistically analyzed by calculating the mean and standard deviation followed by applying paired ‘t’ test to the observational records at interval of zero day, 30th day, 60th day and 90th day.
RESULTS
Socio-demographic characteristics comprised the age, sex, marital status, occupation etc. The observation was that maximum numbers of cases were between 51-60 years of age groups i.e. 15 (Table 1). The higher number of males patients may be due to lack of excises or sedentary work (Table 2). The reason for the predominance of Muslim may either be due to the use of excessive non-vegetarian food, that comprises saturated fats and that raises the concentration of plasma lipids.
After 90 days of treatment from the compound formulation of Unani Medicine i.e. Sharbat-e-Qalbi exhibited significant decrease in the level of complete lipid profile. Statically Paired ‘t’ test is highly significant in lipid profile, like Cholesterol, Triglycerides, LDL and HDL (Table 3).
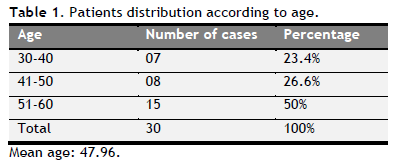 |
Table 1. Patients distribution according to age. Click here to view full image |
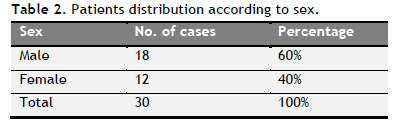 |
Table 2. Patients distribution according to sex. Click here to view full image |
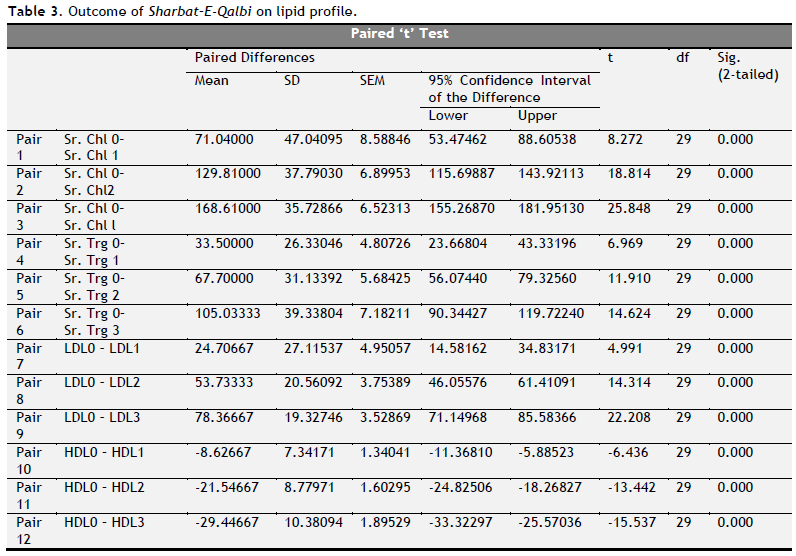 |
Table 3. Outcome of Sharbat–E-Qalbi on lipid profile. Click here to view full image |
DISCUSSION
Hyperlipidemia in combination with abnormally low concentrations of HDL cholesterol (High Density Lipoprotein Cholesterol) is one of the most common and atherogenic pro-file of lipid metabolism of high prevalence seen in Indian population (Rissam et al., 2001; Ansarullah et al., 2009; Grundy et al., 2004; LaRosa et al., 1990).
The study shows that maximum numbers of cases were in the age group of (51–60) and male are more prone to this disease in contrast to female. It may be due to inappropriate diet with life style; again in India male persons are busy with their work and less conscious about their health. The reason behind predominance of Muslim may either be due to the use of excessive non vegetarian diet, which contains saturated fats and that increases the concentration of plasma lipids.
In the study it was observed that after 90 days of treatment from the compound formulation of Unani Medicine i.e., Sharbat-e-Qalbi showed substantial decrease observed in cholesterol, triglyceride, HDL, LDL & VLDL in serum.
Our results about the changes in LDL and HDL are very important because data from different study showed that for a given level of LDL, the threat of heart disease rises 10-fold as the HDL varies on or after high to low. While, for a fixed level of HDL, the danger rises 3-fold as LDL varies after low to high. It is also witnessed that higher level of HDL (over 60 mg/dL) have protective value against cardiovascular diseases such as ischemic stroke and myocardial infarction. Lower levels of HDL (under 40 mg/dl for men, under 50 mg/dl for women) is a affirmative risk factor for these atherosclerotic ailments (Thorne, 1998).
CONCLUSION
It may be concluded that the effect of the test combination of drugs in lowering the serum level of cholesterol, triglycerides, LDL and in increasing the level of HDL. The medicine was well accepted with negligible side effects; consequently it is beneficial for the patients of hyperlipidemia, atherosclerotic illnesses for preventive aspect as well as therapeutics. Further studies at advanced level will be carried out on more number of patients to get this drug for patent.
CONFLICT OF INTEREST
None declared.
REFERENCES
Abdul Nasir et al. ‘Hyperlipidemia (Fart-e- tadassum fid –dam) in the light of Unani System of Medicine’, Published by International Pharmaceutica Science. 2013;3(4):1-8.
Allama Hakim Najamul Ghani Rampuri, Khazainul Advia, 3rd Edition, Jan 2011, Idara Kitabus shifa, New Delhi. Page no’s: Adrak: 211-212, Laisan: 1197-1199, Lemu: 1201-1203, Sirka &Seeb: 802-804,877-879, and Shahed: 918-920.
Ansarullah, RN Jadeja, MC et al. Antihyperlipidemic potential of a polyherbal preparation on triton WR 1339 (Tyloxapol) induced hyperlipidemia: A comparison with lovastatin. International Journal Green Pharmacy. 2009; 3(2):119- 124.
Boyer Rodney, Concept in Biochemistry, 2nd edition (The Wadsworth Group Library of Congress, USA); 2002.
Cristie M. Ballantyne & Rone Hoogreen, Role of Lipids and lipoprotein profile in risk assessment & therapy. American Heart Journal. 2003;146:228.
Grundy SM, Cleeman JI, Merz CN et al. Implications of recent clinical trials for the national cholesterol education programme adult treatment panel III guidelines. Circulation, 2004;110:227-239.
Hakeem Mohammed Bin Zakariya Razi, ‘Alhawi- fit-tibb’ Urdu Translated CCRIUM, New Delhi, India; 1999.
Hakim Kabiruddin, Magzanul Mufridath, 2000, Faisal Brothers, New Delhi. Page no’s: Adrak: 366-367, Laisan: 519-521, Lemu: 521-523, Sirka & Seeb: 342-343,371-373 and Shahed: 389-390.
Hakim Mohammed Abdul Hakim, Butanul Mufridath, 2002, Idara Kitab ul shifa, New Delhi. Page no’s: Adrak: 60, Laisan: 526-527, Lemu: 528-529, Sirka & Seeb: 335-337,565-567 and Shahed: 384-385.
Hkm Kabeeruddin, Bayaz-e Kabeer, Vol 3, 5th edition, Eijaz Publication House, New Delhi, India; 1935.
Ibn Sina, Al qanoon-fit tibb,translated by Ghulam Husain Kitnoori, Idara Kitab-us-shifa, kucha Chelan, Darya Ganj, New Delhi, India; 2010.
LaRosa JC, Hunninghake D, Bush D, Criqui MH, Getz GS, Gotto AM, et al. The cholesterol facts. A summary of the evidence relating dietary fats, serum cholesterol and coronary heart disease. A joint statement by the American Heart Association and National Heart, Lung and Blood Institute. The task Force on Cholesterol Issues, American Heart Association. Circulation. 1990;81:1721-1733.
Nafees B, ‘Kulliyat-e-Nafeesi’, Part-1, Tarjuma wa Sharah, Hkm Kabeeruddin, Matba Daftarul Maseeh, Hyderbad 1954: 28 -86.
Nafees B, Moalijat-e-Nafeesi, Munshi Nawal Kishor, Lucknow 1906: 538-540.
Rihana Kamal, Shagufta Aleem. Clinical evaluation of efficacy of a combination of zanjabeel (Zingiber officinale) & amla (Emblica officinale) in hyperlipidemia. Indian Journal of Traditional Knowledge. 2009;8(3):413-416.
Rissam HS, Kishore S, Trehan N. Coronary Artery Disease in Young Indians–The Missing Link. Journal, Indian Academy of Clinical Medicine. 2001;2(3):128-132.
Schaefer JR. Drug therapy of hyperlipidemia. Current status in Germany. “Dyslipdemia”. Lancet. 2003; 362 (9385): 717–31.
Thorne S, Mullen MJ, Clarkson P, Donald AE, Dean field, JE. Early endothelial dysfunction in adults at risk from atherosclerosis: different responses to l-arginine free. Journal of the American College of Cardiology.1998;32(1):110-116.
Ziur-Rehman, Kitabul Murakabat, AMU, Aligarh, 2nd Edition, Eijaz Publication House, New Delhi, India; 1991.
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.