






Abdul Nasir1*, Mohd. Akhtar Siddiqui2, Mohd. Aftab Ahmad3, Gazala Fatma4
1Majeedia Unani Hospital, F/o Medicine (U), Jamia Hamdard, New Delhi-62 India.
2Department of Moalijat, F/o Medicine (U), Jamia Hamdard, New Delhi-62 India.
3Department of Ilmul Advia, F/o Medicine (U), Jamia Hamdard, New Delhi-62, India.
4Faculty of Medicine Unani, Jamia Hamdard, Hamdard Nagar, New Delhi-62, India.
REVIEW ARTICLE
Volume 4, Issue 1, Page 29-33, January-April 2016.
Article history
Received: 10 March 2016
Revised: 25 March 2016
Accepted: 10 April 2016
Early view: 25 April 2016
*Author for correspondence
E-mail: [email protected]
Eczema (Nar-e-farsi) is an inflammatory responsive condition of the skin which is characterized by erythema, skin edema, vesiculation, itching, oozing or bleeding, flaking, blistering, cracking, crusting and lichenification. Although many theories are bound to explain etiology. But basically two factors causing eczema are described. Firstly an allergic or sensitive skin and secondly exposure to an irritant. However the following factors are described: age, genetic predisposition, climate, debility, psychological factors, exciting factors like soaps, polish, hair dye, colours, cream, Hand bags, slippers, penicillin, iodine, streptomycin, bacteria, virus, and fungus. Several Unani single drugs like Shahtra (Fumaria indica Pugsley), Chiraita (Swertia chirayita Roxb.), Sarphoka (Tephrosia purpurea Linn.), Gul-e-mundi (Sphaeranthus indicus Linn.) and Unnab (Ziziphus jujuba Mill.) etc. as well as compound drugs like Qurs Musaffi Khoon, Majoon Ushba, Sharbat Musaffi Murakkab, Sharbat Unnab, Sharbat Nilofer, Arq-e-Shahatra, Arq-e-Mundi etc. The present paper shows brief description like introduction, eitiology, pathophysiology, classification, clinical features, investigation, differential diagnosis, diagnosis, complications and management of Eczema (Nar-e-farsi) in modern and Greek medicine.
Keywords: Eczema, Nar-e-farsi, Chhajan.
INTRODUCTION
The term eczema comes from Greek word means ‘to boil out’(ec=out; zema=boil) because in eczema skin is boiling out or oozing out. The term dermatitis also comes from Greek word for inflammation of skin. Among some people eczema and dermatitis are synonyms while among other people dermatitis implies an acute condition and eczema is a chronic one, so it is clear that all eczema are dermatitis but not all dermatitis are eczema (Hunter & Savin 2003, Khanna 2008).
According to Ibne Abi Sadique ‘Nar-e-farsi’ is named because Naar = means ‘Aag’ a patient feel more irritation and burning sensation in those lesions, Farsi= means ‘it was more common among people of Persia (Mulk Faras) or refered to the physicians who treat the Nar-e-farsi first also was a resident of Persia (Mulk Faras) (Kirmani 2012).
Nar-e-farsi is a dermatological disorder which is well known since Greeco-Arab period. Unani Physicians not only described the normal structure and functions of skin but also mentioned the eitiology, pathophysiology, clinical pictures, line of treatment (Usool-e-Ilaaj) and management of various skin disease. Unani scholars have described the Nar-e-farsi (Eczema) in detail along with meaning, eitiology (Asbaab), pathophysiology (Maahiyat), Aqsaam (Types), clinical pictures (Alamat) and management (Ilaaj) (Kirmani 2012, Sina 2010).
Synonyms: Nar-e-farsi, Chhajan, Akota
Pathophysiology (Maahiyat)
According to Unani physician ‘Nar-e-farsi’ is a skin disease, in which rashes at the site of lesions occur and shows peacock shaped linear flame of fire. After some time vesicles formation (Muratab dane) along with irritation and severe itching occur (Kirmani 2012). In a later stage these vesicles ruptured and changed into dry state and finally crust formation and lichenification occur (Chandpuri 1998).
According to modern physicians the characteristic change is oedema between the cells of the epidermis, known as spongiosus, leading to formation of vesicles. The whole epidermis becomes thickened with an increased keratin layer. A variable degree of vasodilatation in the dermis and an inflammatory infiltrate may be present. They may vary according to the type of eczema. The pathogenesis of exogenous eczema, particularly primary irritant and allergic contact eczema is well understood, but that of endogenous eczema is not yet very clear (Buxton 2003).
Eitiology (Asbab)
Unani scholars have described the causes of Nar-e-farsi are:
Mixing of khilt-e-Safra into blood, indigestion, general weakness, nerve weakness, arthritis, gout, intestinal worms, incomplete evacuation, use of garlic, mustard, chilly, spicy food and extreme hot or cold (Aleem 2014, Kirmani 2012).
In modern medicine basically two factors causing eczema are described. Firstly an allergic or sensitive skin and secondly exposure to an irritant, however the following factors are described (Hunter & Savin 2003, Buxton 2003):
• Age: Atopic eczema begins in the first 2 years of life. Seborrheic eczema is a problem of elderly person, discoid eczema and nummuler eczema are most common in the middle age.(Goldman 2000)
• Familial predisposition: Genetic predisposition is responsible for the preponderance of eczema in certain families. Atopic eczema is the best example.
• Climate: Climate condition like extreme heat, dampness and severe cold.
• Debility: General physical debility plays an important role in the occurence of eczema.
• Psychological Factors: They are responsible for promotion of the development of any type of eczema e.g. lichen simplex chronicus, mainly seen in tense and anxious middle aged subject of either sex.
• Exciting Factors: (Souhami & Moxham 2002, Kumar & Clark 2006)
(a) Chemicals and minerals: Soaps, polish,Hair dye,
colours, cream etc.
(b) Plastic material: Hand bags, slippers, shoes, strap of watch etc.
(c) Occupation: Washerman, gardener, dyer, cobbler
etc.
(d) Foods: Pork eater, excess use of spices.
(e) Drugs: Penicillin, iodine, streptomycin etc.
(f) Infections: Bacteria, virus, fungus, etc.
Types of eczema (Aqsam of Nar-e-farsi)
Ancient Unani physicians have classified the eczema (Nar-e-farsi) into following types (Sina 2010, Kirmani 2012):
• Depending upon the forms and secretions of the lesions:
o Nar-e-farsi Sada
o Nar-e-farsi Ahmar (Surkhi mael)
o Nar-e-farsi Naffati (Abladar)
o Nar-e-farsi Mutaqaiyah (Peepdar)
o Nar-e-farsi Sulb (Hardness at the site of leison in the skin)
o Nar-e-farsi Shaqaqi (Cracking at the site of leison in the skin)
• Clinically it is divided in the following types:
o Acute Eczema (Nar-e-farsi haad)
o Chronic Eczema (Nar-e-farsi muzmin)
In modern medicine eczema has been classified in the following manner:
• Depending upon the type of leison:
o Acute phase: Erythema, edema, vesiculation, oozing, crusting.
o Sub acute: Hyperpigmentation, scaling and crusting.
o Chronic: Lichenification.
• Now a days eczemas are classified for practical use into two broad groups: (Buxton 2003, Kumar and Clark 2006)
o Exogenous eczema:
(a) Irritant contact eczema
(b) Allergic contact eczema
(c) Photosensetive eczema
(d) Infective eczema
o Endogenous eczema:
(a) Atopic eczema
(b) Seborrheic eczema
(c) Nummular eczema
(d) Asteatolic eczema
(e) Stasis eczema
(f) Dyshidrotic eczema
Clinical Features (Alamat)
Clinical features mentioned in classic literatures are as follows (Nawab et al. 2008, Sina 2010 & Kirmani 2012):
• Skin coloring changes, such as more or less color than the normal skin tone.
• Skin redness or inflammation around the blisters, intense itching and oozing.
• Thickened or leather-like areas (called lichenification), which can occur after long-term irritation and scratching
• The type and location of the rash can depend on the age of the patient:
• It may be in children, elderly and old people but in children younger than 2 years of age, skin lesions begin on the face, scalp, hands, and feet. The rash is often itchy and bubble, ooze, or form crusts.
• In older children and adults, the rash is more often seen on the inside of the knees and elbow. It can also appear on the neck, hands, and feet.
• Rashes may occur anywhere on the body during a bad outbreak.
• Intense itching is common. Itching may start even before the rash appears. Atopic dermatitis is often called the “itch that rashes” because the itching starts, and then the skin rash follows as a result of scratching.
In short clinical features depend on the stages of eczema:
1. Acute Eczema
This is characterized by plaque which are ill defined, erythematous and edematous, surmounted by papules and vesicles which on rupturing show the lesion an oozy look, exudates dries to form crusts, scaly and spongiosis.
2. Chronic Eczema
In chronic condition there may be less exudation, scaling which may be prominent, lichenification (It means triad of hyperpig-mentation, thickening of skin and increased skin markings) and fissuring in flexural lesions.(Hunter & Savin 2003)
Investigations (Tafteeshat):
1. Patch Tests (Hunter & Savin 2003, Goldman 2000) and Schofield 2007):
Patch tests detect type IV hypersensitivity (delayed). A standard european battery of common allergens such as nickel and chromate is applied to the skin of the back under aluminium discs for 48 hours.
2. Prick Tests: (To detect type 1 hypersensitivity), these tests are performed to support the diagnosis of atopic eczema (Buxton 2003).
3. Serological tests: to detect the level of serum IgE and IgE antibodies.
4. Bacterial and viral swabs for Microscopy and Culture:
5. Skin scrapings for Mycology
6. Skin biopsy (rare)
Differential Diagnosis (Khanna 2008, Schofield 2007):
A. Psoriasis Eczema
• Moderately itchy Very itchy
• Scratching promote bleeding It promotes oozing
• Plaques well defined Plaques not so well defined
• Silvery scales May be scale and crust
• Auspitz sign positive Negative
• Typical nail changes Variable nail changes
B. Scabies in infants Infantile Eczema
• Special pattern of lesions on palms It spares
palms, soles & genitalia
• Burrows present Absent
• Same typical lesions in family members May be
atopic diathesis in family
C. Dermatophytic infections Eczema
• Annular lesions (centre clear) Discoid lesions
• Minimal exudation/crusting Exudation,
crusting and lichenification
• Potassium hydroxide Negative
mount for fungal hyphae
shows fungal hyphae
Diagnosis (Tashkhees):
Diagnosis of eczema is based on the following features:
• How the skin looks
• Personal and family history of the patient.
• Allergy skin testing and allergy symptoms skin rashes that form only on certain areas of the body after exposure to a specific chemical may be helpful for diagnosis.
• Itchy exudative plaques, surmounted by papulovesicles.
• Lichenification may be prominent in chronic lesions.
• Skin Biopsy (to rule out any malignancy)
Complications
• Dermatological complications (Khanna 2008):
o Infections of the skin caused by bacteria, fungi, or viruses
o Ide eruption
o Permanent scars
o Contact dermatitis
o Erythroderma
• Psycological complications (Khanna 2008):
o Depression
o Anxiety
o Debility
o Wage loss
o Social ostracism
o Social complication
Management of eczema in Unani medicine
Usool-e-Ilaaj (Principles of treatment) (Aleem 2014, Kirmani 2012):
• Izala-e-Sabab (Treat the cause)
• Tanqiya-e-Muwad (for evacuation of bad elements)
• Musaffiyat-e-Dam (Blood purifier)
• Mana-e-Ufoonat-e-Jild (Antiinfective)
• Musakkinat-e-Jild (Sedative to the skin)
• Mulayyanat wa Mushilaat in case of constipation
• Bathing and cleaning of lesions
Ilaaj Nar-e-farsi (Treatment of eczema) (Sina 2010, Kirmani 2012, Aleem 2014)
Izala-e-Sabab
Treat and remove the cause which is responsible for Nar-e-farsi
Tanqiya-e-Muwad (for evacuation of bad elements)
For this purpose joshanda of Sana makki 5gm, Saqmooniya 5gm, Haleela kabli 5gm, Aaloo Bukhara 5gm can be given to the patient before taking Musaffiyat-e-Dam (Blood purifier)
Musaffiyat-e-Dam (Blood purifier) and Mana-e-Ufoonat-e-Jild (Anti-infective)
• Single drugs Mufradat)
A lot of Unani single drugs like Shahtra (Fumaria indica Pugsley), Chiraita (Swertia chirayita Roxb.) Sarphoka (Tephrosia purpurea Linn.), Gul-e-mundi (Sphaeranthus indicus Linn.), and Unnab (Ziziphus jujuba Mill.) etc.
• Compound drugs (Murakkabat)
There are some compound drugs like Qurs Musaffi Khoon, Majoon Ushba, Sharbat Musaffi Murakkab, Sharbat Unnab, Sharbat Nilofer, Arq-e-Shahatra, Arq-e-Mundi etc. are mostly used in the treatment of Nar-e-farsi.
Musakkinat-e-Jild (Sedative to the skin) and Mana-e-Ufoonat-e-Jild (Antiinfective)
• Dry and crush the leaves of henna (25 gm) and black cumin (25 gm) and mix it with 200 ml of olive oil then heat the mixture till burnt/charred. The mixture should be filtered and filterate contain plastic bottle and apply four times a day on eczematous lesion (Nawab et al. 2008).
• Apply Rasot mixed with Roghan-e-Gul locally
• Apply Marham Safeda Kafoori for sedation
• Apply Sandal, Murdarsang, Kafoor after mixing in Arq-e-Gulab locally.
Mamoolat-e- Matab
• Majoon Ushba 7gm first
And then Joshanda of , Barg-e-Shahatra, Chiraita, Sankhahooli, Unnab, Sandal safed, Sandal surkh, Sarphoka,Gul-e-Nilofer, Mundi with Sharbat Unnab 20 ml twice a day in the morning and evening is given to the patient.
• Jawarish Jalinoos twice a day after meal
• Itrifal Shahatra 10 gm HS
• Marham Safeda Kafoori for L.A
Management in Modern Medicine (Khanna, 2008; Peter, 2013; Kumar & Clark, 2006; Sauhami & Moxham, 2002):
Remove the triggers:
• Aggravating factors/irritants/allergens e.g. avoid scratch -ing the rash or skin, Irritants such as wool and lanolin, alcohol, scents, dyes and other chemicals.
Hydration:
• Keep the skin moist, use ointments (such as petroleum jelly), creams, or lotions 2-3 times a day.
Acute localized lesions:
• Soaks are used followed by topical application of corticosteroids.
Acute extensive lesions:
• There can be used short course of systemic steroids.
Infected lesions:
• In this case topical or systemic antibiotics and topical corticosteroids
Chronic lesions:
• In chronic lesion topical corticosteroids mostly with keratolytic agents like urea and salicylic acid.
Other treatments that may be used in case of eczema include:
• Antihistamine medicines by mouth are used to reduce severe itching.
• Antibiotic creams or pills can be used if the skin is infected
• Those drugs that suppress the immune system, such as cyclosporine, methotrexate, or mycophenolate mofetil
• Phototherapy, a medical treatment in which your skin is carefully exposed to ultraviolet (UV) light.
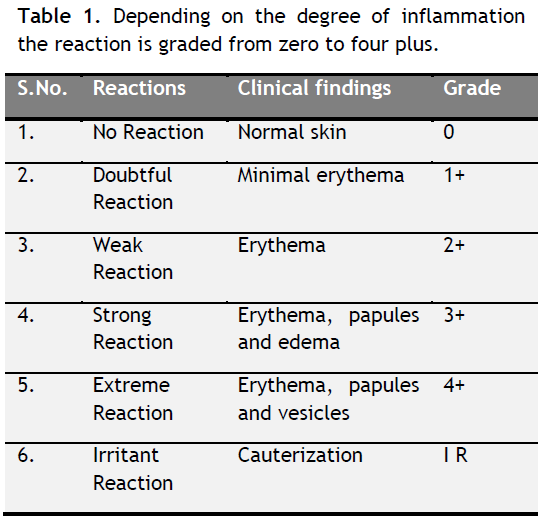 |
Table 1. Depending on the degree of inflammation the reaction is graded from zero to four plus. Click here to view full image |
CONCLUSION
Eczema is not a life threatening disease, it is an inflammatory response to the skin. Ancient Unani physicians have described the eczema in the name of Nar-e-farsi and were well aware about eczema and have described the etiological factor, types, pathology, clinical features in detail. They have also used a lot of single drugs, compound drugs and locally applicable drugs in the management of eczema. But there is need of specific type of herbal drugs in the treatment of eczema along with scientific validation.
CONFLICT OF INTEREST
None declared.
REFERENCES
Aleem Shagufta. Chhajan/Nar-e-farsi: Amraz-e-Jild, Second Edition, Adabistan publications; 2014. P. 86-93.
Buxton Paul K. Eczema and dermatitis: Abc of Dermatology, Fourth Edition BMJ Publishing Group London; 2003. P. 17-19.
Chandpuri Kauser. Jamrah and Nar-e-farsi: Moojizal Qanoon, Third Edition, Qaumi Council Barai Frogh Urdu Zaban; 1998. P. 441.
Hunter JAA, Savin JA, Dahl MV. Eczema and Dermatitis: Clinical Dermatology, Third Edition, Blackwell Publishing; 2003. P. 70-90.
Khanna Neena. Eczematous Dermatitis: Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, 2nd Edition, Elsevier 2008; P. 289-292.
Kirmani Nafees bin Auz. Nar-e-farsi/Eczema: Moalijat Sharah Asbab (Urdu translation by Allama Kabeeruddin) Vol.3, Aijaz Publication House, Darya Ganj, New Delhi; 2012. P. 256-257.
Kumar P, Clark ML. Eczema: Kumar & Clark’s Clinical Medicine, Sixth Edition, Saunders Ltd.; 2006. P. 1326-1331.
Nawab Md, Mannan Abdul. Siddiqui Misbahuddin. Evaluation of the clinical efficacy of Unani formulation on eczema. Indian Journal of Traditional Knowledge. 2008; 7 (2): 341-344.
Parker Frank. The Eczemas (Dermatitis). In: Goldman Lee, Ausiello D, editors. Cecil Text Book of Medicine. 21st edition. Published by Saunders an Imprint of Elsevier; 2000. p. 2276-2279.
Peter D, Arkwright, MB, DPhila, Cassim Motala, MD, Hamsa Subramanian et al. Management of Difficult to treat Atopic Dermatitis. Journal of Allergy Clinical Immunology: In Practice. 2013; 1(2): 142-150.
Schofield OMV, Rees JL. Eczema. In: Boon NA, College NR, Walker BR and Hunter JAA, editors. Davidson’s Principals and Practice of Medicine, 20th Edition, Churchil Livingstone; 2007. P. 1283-1287.
Sina Ibne. Nar-e-farsi: Alqanoon-fit-Tibb translated by Ghulam Husain Kintoori, Idara Kitab-us-Shifa, Kucha Chelan, Darya Ganj, New Delhi; 2010. P. 1260-1261.
Souhami RL, Moxham J. Eczema and Dermatitis: Textbook of Medicine. Fourth Edition, Churchil Livingstone; 2002. P. 399-404.
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.