






Mohammed Abrar Hassan1*, Daya Sagar Reddy2, Mohammed Anwaar Ahmed2
1Department of Physiology, Bhaskar Medical College, Yenkapally, Moinabad, RR (Dist.), AP, India.
2Department of Ophthalmology, Bhaskar Medical College, Yenkapally, Moinabad, RR (Dist.), AP, India.
ORIGINAL RESEARCH ARTICLE
Volume 2, Issue 1, jan-April 2014.
Article history
Received: 01 March 2014
Revised: 20 March 2014
Accepted: 25 April 2014
Early view: 28 April 2014
*Author for correspondence
E-mail: [email protected]
Mobile/ Tel.: 000000000
keywords:
Myopia
Ammetropia
Keratometry.
The present study was conducted in view of increasing incidence of refractive error in rural patients attending the ophthalmic clinics particularly. This study was done exclusively to identify the prevalence of myopia in rural population. The type of myopia, the incidence of myopia varied in different age groups. The present study showed that there was a high prevalence of myopia in younger age group in axial type while the older age group showed predilection towards index myopia. This shows the prevalence of myopia was significant in rural population but the correction varied. While the middle aged group had almost equal subjects in axial and index category with fully developed cataractous opacities.
INTRODUCTION
The present study was conducted in view of increasing incidence of refractive error in rural patients attending the ophthalmic clinics particularly. Myopia being viewed as leading cause of all ammetropic eyes, patients from all walks of life is complaining of diminished vision, involving both adults and children. The reason for spurt in myopic patients could be due to increase exposure to audio and visual stimuli like television computer and video games viewing , mobile phone which has become a necessity and as well pass time play for all age group. Academic competitive life has encroached the rural population for excellence in every field. People are enjoying under entertainment source without having control over the hours spent on audio visual stimuli (Batra et al., 2007).
Myopia is the commonest eye disorder in humans around the world; it has affected 25-35% of adult population in the world. There is a debate on role of genetics in the development of myopia. Some believe that myopia may be inherited but actually the disorder results from a combination of environmental and genetic factor, and other factors. The demographic distribution of myopia is higher due to income level and education. The prevalence of myopia is higher among people with above average income in people whose work require great deal of close focusing or near work. Various studies showed the prevalence of myopia in school children; a study in India reported 20% of myopia (Murray et al., 1996), in Jordan 17.6% (Khader et al., 2006), in Iran showed 3.8% prevalence of refractive error (Fotouhi et al., 2007), while a study in Malaysia reported 17.1 % prevalence of refractive error and 9.6% myopia (Khader et al., 2006). Due to modernization of village and change in dietary habits and life style ammetropia is increasing in rural population (Fledelius, 2000). This study is planned to access the myopia status in rural population.
CASE REPORT
This was a prospective study, conducted on 100 patient attending department of ophthalmology as out-patients at Bhaskar Medical College, Moinabad, AP, India for refractive error correction. The subjects were divided into three groups based on age group of 10-60 years; group A–10-20 years, group B–21 to 40 years, group C- 41-60 years.
After obtaining permission from Institutional Ethic committee, a voluntary written informed consent was obtained on prescribed pro forma made as per ethical norms. Slit lamp examination were performed to rule out the status of lenticular opacification and corneal curvature. The refractive status was assessed by subjective and objective assessment using auto-refractometer, confirmed by streak retinoscopy. Keratometry was done for corneal curvature defects. A scan biometry for axial length was performed. The results analyzed for statistical significance for P-value using Paired t-test. The myopic patients attending the ophthalmology OPD were included in this study while all
the other types of refractive error were excluded and also diseases like uveitis, glaucoma were not included.
DISCUSSION
This study was done exclusively to identify the prevalence of myopia in rural population. The type of myopia, the incidence of myopia varies in different age groups. In group A, the myopic population was maximum with 44% with keratoconus. This group had almost all the subjects belonging to axial type of myopia as the A scan values were falling in the range of 25- 30 mm while the K values were in the range of 38-40 excepting 1 subject with huge difference falling in curvature type of myopia. While in -3.25 Dsph and above range, the prevalence of ammetropia was higher in rural children i.e. about 11.53% and urban children was about 5.35%. In group B, the total numbers of cases were 38%. This group had 20 cases of axial myopia with the A scan values falling in 25- 30 mm, while the remaining 18 subjects showed the occurrence of lenticular opacification that mean the cause of myopia could be due to change in refractive index towards myopic side. In group C, There were only 18% subjects falling in index myopic category with fully developed cataractous opacities and responding to–3.00 to 5.00 D of corrections. A scan showed lenticular spikes.
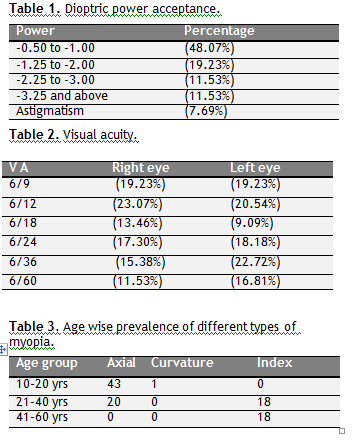 |
Table 1,2 & 3 Dioptric power acceptance Visual acuity and Age wise prevalence of different types of myopia. Click here to view full image |
The refractive error was corrected with spectacles bearing the power between the range of -0.5 to -3.00 and above with highest subjects accepting -0.5 to 1.00 D (48.07%), 19.23% accepted -1.25 to -2.00 D, 11.53% accepted -2.25 to -3.00 D, 11.53% where above -3.00 D. While 7.68% were having astigmatism. The visual acuity affected was in 23.07% subjects having 6/12 while about 11.53% subjects had visual acuity less than 6/60.
CONCLUSION
This study showed that there is a high prevalence of myopia in younger age group in axial type while the older age group showed predilection towards index myopia. This shows the prevalence of myopia is significant in rural population but the correction varies while the middle aged group had almost equal subjects in axial and index category.
CONFLICT OF INTEREST
None declared.
REFERENCES
Batra N, Kaushal D, Gill AS. Refractive errors in school children-Data from a school. Tropical Ophthalmology. 7, 43-47, 2007.
Fledelius HC. Myopia profile in Copenhagen medical students 1996-98. Refractive stability over a century is suggested. Acta Ophthalmol Scand. 78, 501-505, 2000.
Fotouhi A, Hashemi H, Khabazkhoob M, Mohammad K. The prevalence of refractive errors among school children in Dezful, Iran. Br J Ophthalmol. 91, 287–292, 2007.
Khader YS, Batayha WQ, Abdul-Aziz SM, Al-Shiekh-Khalil MI. Prevalence and risk indicators of myopia among school children in Amman, Jordan. East Mediterr Health J. 12, 434-439, 2006.
Murray CJ, Lopez AD. The Global Burden of Disease: a comprehensive assessment of mortality and disability from diseases, injuries and risk factors in 1990 and projected to 2020. Cambridge, MA, Harvard School of Public Health,
(Global Burden of Disease and Injury Series, vol I), 1996.
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.